Zygomatic Fractures
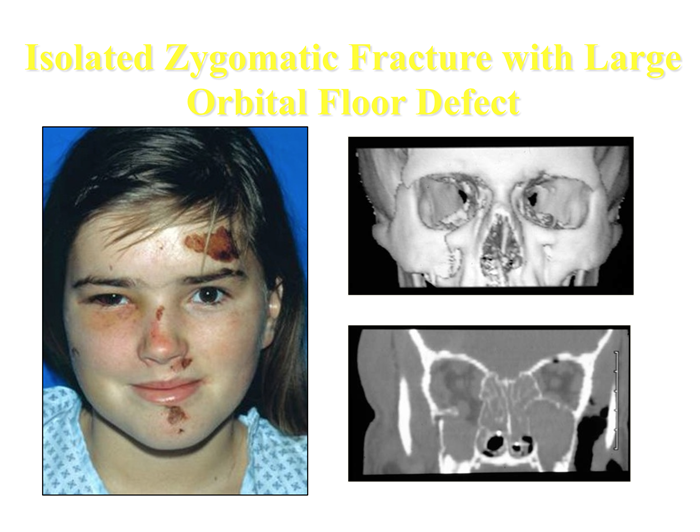
The zygomatic bone occupies a prominent and important position in the facial skeleton. It plays a key role in determining facial width as well as acting as a major buttress of the midface. Its anterior projection forms the malar eminence and is often referred to as the malar bone. The zygoma has several important articulations in the midface. The zygoma forms a significant portion of the floor and lateral wall of the orbit. In addition, the zygoma meets the lateral skull to form the zygomatic arch. The zygoma is the main buttress between the maxilla and the skull; but in spite of its sturdiness, its prominent location makes it prone to fracture. The mechanism of injury usually involves a blow to the side of the face from a fist, object, or secondary to motor vehicle accidents. Moderate force may result in minimally or nondisplaced fractures at the suture lines. More severe blows frequently result in inferior, medial, and posterior displacement of the zygoma. Comminuted fractures of the body with separation at the suture lines are most often the result of high-velocity motor vehicle accidents. In general, displaced fractures will involve the inferior orbital rim and orbital floor, the zygomaticofrontal suture, the zygomaticomaxillary buttress, and the zygomatic arch. Occasionally, however, a direct blow to the arch will result in an isolated depressed fracture of the arch only.
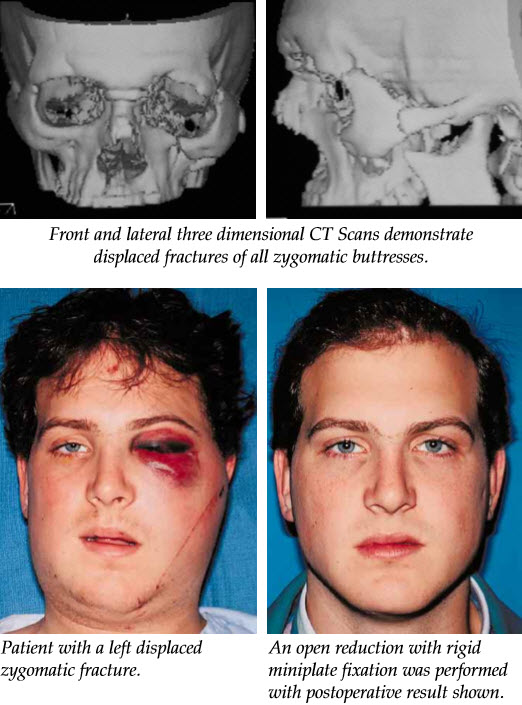
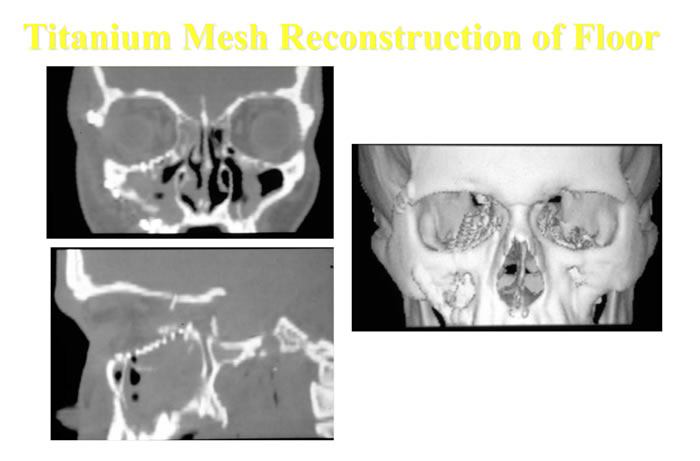
Radiographic evaluation of the fracture is mandatory and may include both plain films and a computed tomographic (CT) scan. The CT scan has now essentially replaced plain films as the gold standard in both evaluation and treatment planning. If physical findings and plain films are not suggestive of a zygomatic fracture, the evaluation may end here. However, if they do suggest fracture, a coronal and axial CT scan should be obtained. The CT scan will accurately reveal the extent of orbital involvement, as well as degree of displacement of the fractures. This study is vital for planning the operative approach.
Historically, closed reduction was the method of choice for nearly all zygomatic fractures. Multiple methods were employed, but most involved simply exerting pressure underneath the malar eminence and popping the fragments back into alignment. Not only were these results frequently unsatisfactory, but they were fraught with complications including persistent diplopia, orbital dystopia, malunion, and significant residual deformity. In our own experience, closed reductions yield unpredictable results with significant chance of relapse. We feel that plate and screw fixation is now the standard of care.

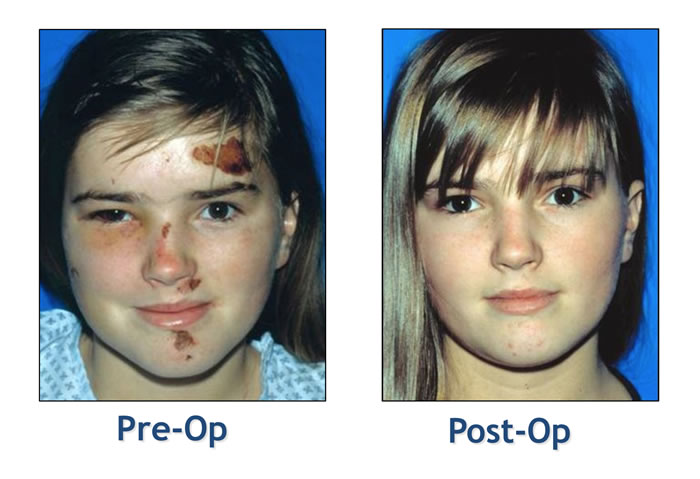
The treatment of zygomatic fractures has dramatically progressed over the past several decades from an entirely closed approach to the more aggressive open reduction and rigid miniplate fixation of today. If a zygomatic fracture is displaced, we do an open reduction and rigid stabilization with mini-and microplates. The floor of the orbit is routinely explored and reconstructed, if needed, to restore orbital volume. The complications of an inadequately or unreduced zygomatic fracture are very difficult to correct secondarily and usually avoidable. We feel that early diagnosis combined with this aggressive surgical treatment yields the best results.
Click here to read more about Incidence and Management of Zygomatic Factures at a Level 1 Trauma Center