Nasoethmoid Fractures
Trauma to the central midface frequently results in fractures of the nasoethmoid orbital (NOE) skeleton. This complex area consists of a union of bones from the nose, orbits, maxilla, and cranium. These fractures may be the most difficult and challenging of all facial fractures to diagnose and treat. To the inexperienced examiner, NOE fractures may be misdiagnosed as simple nasal fractures, and a high degree of suspicion is necessary to make the diagnosis. These fractures may occur as isolated injuries or as part of more complex (LeFort) facial fractures. Swelling of the nose and medial canthal areas may mask the fractures and make the physical findings obscure. Failure to diagnose these injuries or inadequate treatment will result in both functional and cosmetic deformities that are very difficult to correct secondarily.

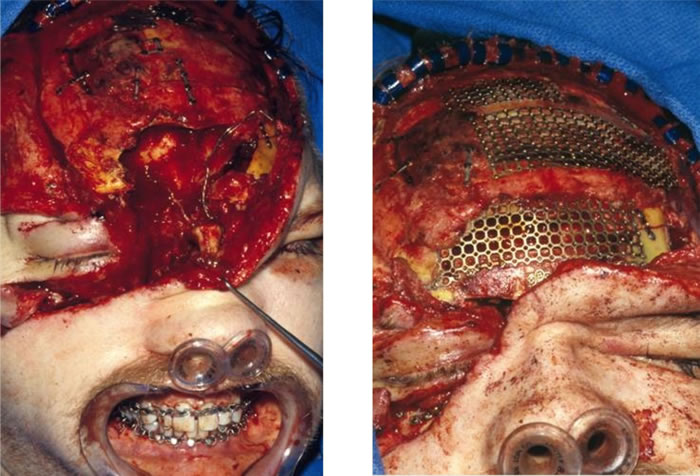



The successful surgical treatment of these complex injuries consist of early open repair with precise reduction and stabilization of bone fragments. Bone grafts are used to restore contour and support to areas of extremely comminuted or missing bone. Soft tissue management of the naso-orbital area is crucial to restoration of preinjury appearance. The application of craniofacial techniques in recent years has greatly enhanced the results now obtainable.
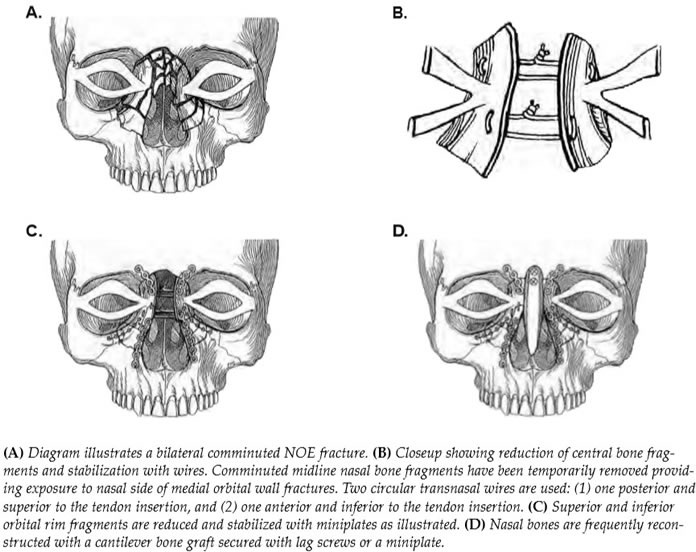
The nasoethmoid region is an intricate confluence of bones that makes up the complex anatomy of the central-upper midface. Identifying and understanding the structural buttresses are crucial to restoring the normal anatomy and appearance of the region. By definition, the nasoethmoid fracture involves disruption of the inferior orbital rim, lateral nasal bones, medial orbital wall, and frontal process of the maxilla. Essentially the medial orbital rim buttress to which the medial canthal tendon is attached is dislocated. It is the operative reduction and stabilization of this central segment of bone that is the key to successful treatment of this injury.
There are a number of potential pitfalls in the surgical treatment of NOE fractures. Once this injury has been diagnosed, the extent of the fracture is determined by physical exam and the CT scan. A definitive early open reduction with stabilization of the fractures utilizing the techniques of craniofacial surgery is then accomplished.

The best results of the NOE fracture are obtained with early diagnosis and aggressive surgical treatment. Complications result when this injury has been misdiagnosed or inadequately treated. Unstable or displaced fractures that are left untreated result in permanent deformities once healed. Late reconstruction is a difficult task that requires repositioning of both bone and soft tissue.
Incomplete reduction of the medial orbital rim fragment, which contains the canthal tendon, can result in a widening of the interorbital distance or a telecanthus. Asymmetric repair, inadequate stabilization, and inadvertent stripping of the medial canthal tendon can all contribute to this problem. Inaccurate assessment of the nasal bones and septal support can lead to contour deformity of the nose with inadequate tip projection. Close attention is needed for reconstruction of the orbital wall fracture to avoid the enlargement of the orbital volume and resultant enophthalmos and vertical orbital dystopia. Although late reconstruction of these deformities is possible, in general, the best aesthetic results are obtained with definitive repair at the time of injury, avoiding the common pitfalls.