HemiFacial Microsomia
The term hemifacial microsomia (HFM) is used to describe a spectrum of complex anomalies characterized by underdevelopment of one side of the face. A variety of terms have been used to identify these facial deformities that result from a developmental malformation of the first and second branchial arches. Such names as craniofacial microsomia, lateral facial dysplasia, first and second branchial arch syndrome, and oculoauriculovertebral dysplasia (Goldenhar’s syndrome) have been used to describe this syndrome.


The incidence of HFM is in the range of 1 in 3500 to 4500. The cause of this deformity has not been satisfactorily identified to date. Transmission is usually sporadic, however, reports do exist of the syndrome being inherited. HFM may occur by itself or in association with other anomalies such as Goldenhar’s syndrome (oculoauriculovertebral dysplasia). Goldenhar’s includes, in addition to a HFM, a bony malformation of the spine and superficial eye lesions called epibulbar dermoids.
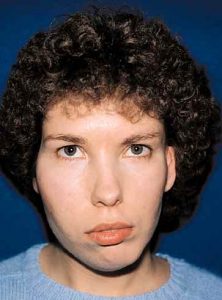
The collected group of deformities that make up this syndrome may vary greatly in extent and degree covering a wide spectrum ranging from mild underdevelopment of the lower jaw to severe deformity of the skull and face. Characteristically this deformity, as the name implies (hemifacial), involves one side of the face, however involvement of both sides to some degree can be observed in as high as 15% of all cases. The most obvious deformity involves the lower jaw and ear, but soft tissue deficiency, maxillary hypoplasia and even orbit and skull anomalies may also be present. Lack of development of the external ear is a common feature with the severity of the ear deformity proportional to the jaw deformity.


These complex problems require a thorough evaluation by the craniofacial team. When we see these patients as infants they are classified according to the severity of the mandibular deformity. Subsequent treatment is individualized being based on this classification and their age at time of evaluation. The goals of treatment are to re-establish facial symmetry (bony and soft tissue), normal occlusion, and hopefully normal joint function. There is some controversy concerning the age in which surgical intervention should be started, however we recommend early surgical correction. In patients born with absent structures, reconstruction of the jaw joint is begun early (before age 6). Children with mild deformities may benefit from the use of an orthodontic device (activator) that attempts to stimulate mandibular growth.
Soft tissue augmentation is performed when necessary after bony skeletal symmetry has been obtained. Ear construction is usually performed at 5-6 years of age. However, in cases of HFM with marked asymmetry of the lower face, ear construction is delayed until bony symmetry is obtained so that the appropriate position of the new ear can be determined.
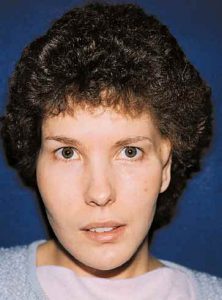
It is important to remember that HFM is a progressive bony and soft tissue deformity with the earliest and most consistent abnormalities noted in the mandible. In general, we recommend early surgical intervention in an attempt to maximize normal growth forces, minimize secondary deformities, and give the patient the psychological benefits that result from early improved appearance and self esteem.